치매의 진단
병리학적으로는 neuritic plaque, neurofibrillary tangle 두 가지 병리 소견을 특징으로
환자의 인지장애가 일상생활의 지장을 초래할 때 진단 가능
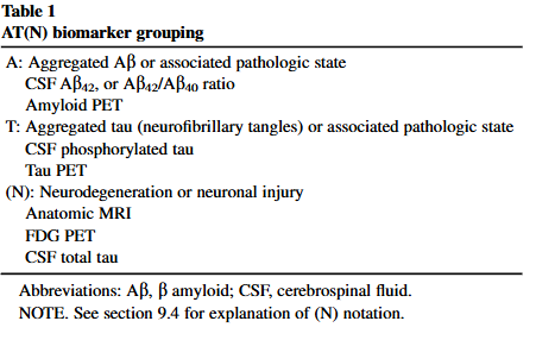
인지장애 + ADL 이상으로만 진단하는건 정확도가 낮아 2018년 NIA-AA (National Institute on Aging and the Alzheimer's Association (NIA-AA) guidelines) Guideline (ATN grouping) 도입
A : Amyloid deposition, T : Tau, N : Neurodegeneration
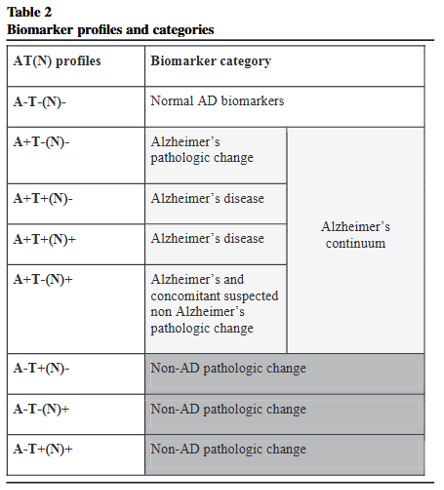
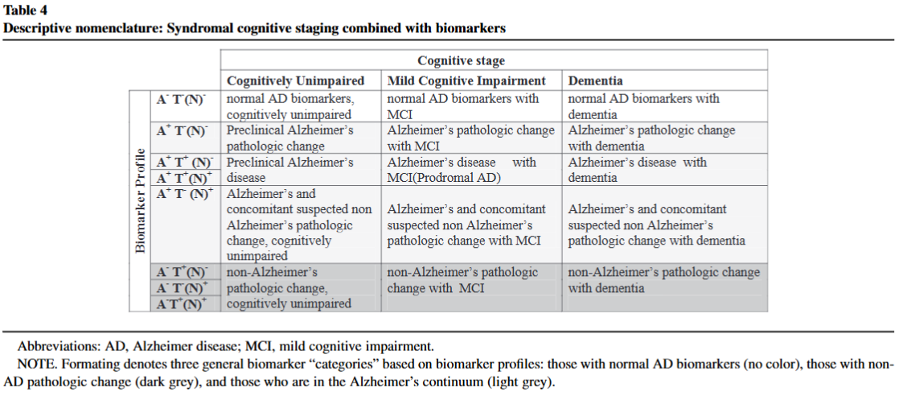
N 없어도 A+T+ 면 AD로 진단가능 (N은 보조적 느낌)
A+T-N+ 는 Alzheimer’s and concomitant suspected non-Alzheimer’s pathologic change
대신 A-T+N+ 는 Non-AD pathologic change
아무튼 Amyloid deposition은 필수적이다!


#Criteria for all-cause dementia: Core clinical criteria
Dementia is diagnosed when there are cognitive or behavioral (neuropsychiatric) symptoms that: 1. Interfere with the ability to function at work or at usual activities; and 2. Represent a decline from previous levels of functioning and performing; and 3. Are not explained by delirium or major psychiatric disorder; 4. Cognitive impairment is detected and diagnosed through a combination of (1) history-taking from the patient and a knowledgeable informant and (2) an objective cognitive assessment, either a “bedside” mental status examination or neuropsychological testing. Neuropsychological testing should be performed when the routine history and bedside mental status examination cannot provide a confident diagnosis. 5. The cognitive or behavioral impairment involves a minimum of two of the following domains: a. Impaired ability to acquire and remember new information—symptoms include: repetitive questions or conversations, misplacing personal belongings, forgetting events or appointments, getting lost on a familiar route. b. Impaired reasoning and handling of complex tasks, poor judgment— symptoms include: poor understanding of safety risks, inability to manage finances, poor decision-making ability, inability to plan complex or sequential activities. c. Impaired visuospatial abilities—symptoms include: inability to recognize faces or common objects or to find objects in direct view despite good acuity, inability to operate simple implements, or orient clothing to the body. d. Impaired language functions (speaking, reading, writing)—symptoms include: difficulty thinking of common words while speaking, hesitations; speech, spelling, and writing errors. e. Changes in personality, behavior, or comportment—symptoms include: uncharacteristic mood fluctuations such as agitation, impaired motivation, initiative, apathy, loss of drive, social withdrawal, decreased interest in previous activities, loss of empathy, compulsive or obsessive behaviors, socially unacceptable behaviors. The differentiation of dementia from MCI (see companion article [5] on the diagnosis of MCI) rests on the determination of whether or not there is significant interference in the ability to function at work or in usual daily activities. This is inherently a clinical judgment made by a skilled clinician on the basis of the individual circumstances of the patient and the description of daily affairs of the patient obtained from the patient and from a knowledgeable informant. (2011 NIH-AA Guideline)
2011년 NIA guideline에서의 criteria에서는 domain에 대해 자세한 설명을 다루고 있다.
여기서 요약하면 ADL에 영향을 주면서, 총 5개 Domain (memory impairment, reasoning and judgement, visuospatial impairment, language difficulties, personality and behavior changes) 중 2개 이상의 domain에서의 cognitive or behavioral impairment가 확인되면 dementia로 진단할 수 있다.
앞선 2018년 NIA-AA guideline의 정의와 비교하면 clinical한 기준이며 단순히 memory impairment 만 관여하지 않더라도 치매 진단을 할 수 있는 중요한 근거로 쓰인다.
'의학공부' 카테고리의 다른 글
| 치매의 약물치료과 급여기준 (0) | 2025.06.15 |
|---|---|
| CDR 계산하기 (3) | 2025.06.15 |
| 🩺 DNR로는 부족합니다 — 요양병원에서 꼭 알아야 할 연명의료결정제도 총정리 (3) | 2025.06.14 |
| 🧠 알츠하이머 치매 : Amyloid-β, Tau의 정상 기능부터 병리 변화, 그리고 p-tau217의 진단적 가치까지 (0) | 2025.06.09 |
| 🧠 아밀로이드-베타와 타우, 왜 함께 다뤄야 하는가?- 치매 치료의 본격적인 변곡점 (1) | 2025.06.09 |




댓글